The joints experience the dynamic environment (load, speed), thus the various mode of lubrication mechanism can exist. However, number of lubricating mechanism has been proposed over the time such as weeping/squeeze film, boosted, boundary, elasthydrodynamic, micro-elastohydrodynamic, and mixed [1]–[3]. Friction and wear of any tribological systems can be influenced by the materials property, surface properties, operating conditions and the environment[4]. Since synovial joints are among the complex and sophisticated tribological systems, so it is likely that many mode of lubrication mechanisms are present.
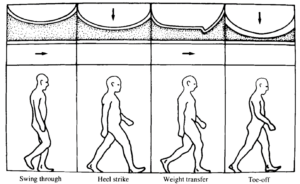
If anyone walks, the interface might be lubricated with synovial fluid via the number of processes such as hydrodynamic, squeeze film/weeping, etc by supporting the load wherever it can. The synovial fluid is squeezed out under loading and consequently lubricates the articular cartilage during off loading(see figure 1). Some of the studies suggest that the synovial fluid cannot separate the articulating surface all the time [5]. When a synovial joint experience the continuous load such as standing for a longer duration, all the fluid is squeezed out of the contact and the load bearing surfaces experiences the boundary lubrication mechanism where the two articulating surface rub with each other. Thus, it can be concluded that synovial joints can encounter the fluild-film, mixed and boundary lubrication similar to the engineering bearings[1]. Murakami et al. [6] termed it as a ‘adaptive multimode lubrication’. The main three mechanism widely studied after their introduction are biphasic lubrication (a form of full film lubrication, since introduced by Mow et al. [7], electrohydrodynamic lubrication (since introduced by Dowson) and brush lubrication(a form of boundary lubrication, since introduced by Hardy et al. [8].
There is limited information on the lubrication mechanism on the artificial total joint replacement. Lubrication mechanism in artificial joints have more variables than the natural synovial joints such as material used, design, contact conditions, patient specific factors, surgical factors etc. Many designers believed that the full film lubrication is difficult to achieve so the efforts have been made towards the improvement in boundary and dry lubricated wear behaviour of implants[9], [10]. Based on the boundary lubrication theory, Charnley[11] developed the low friction arthroplasty using UHMWPE as the acetabular cup combined with the stainless steel femoral head in total hip replacement resulting low wear. In addition to this, various implant design were proposed based on fluid film, elasto-hydrodynamic, elasto-mixed etc[1].
Suitable selection of design parameters (head diameter, diametral clearance etc.) promotes the contact to undergo full hydrodynamic lubrication in hard/hard bearings implants[12]. For instance, when the head diameter is small(16 to 22.5 mm) the surface is under boundary lubrication regime, and when the head diameter is 28 mm it is under mixed lubrication regime[13]. This is because of the tendency to provide surface separation for considerable amount of gait cycle and hence evidence of lubricating film formation. Also, with the increase in the diameter results in higher sliding area which will increase the wear under boundry or mixed lubrication regime. To conclude, it is obvious that the all boundary, mixed and elasto-hydrodynamic lubrication mechanism have been supported by the past studies but most of the implants likely experienced mixed lubrication regimes more than other two. Continuous studies are being carried out in order to mimic the natural synovial joints which undergoes full range of conditions.

This article was written by Dilesh Raj Shrestha as part of an ongoing series of scientific communications written and curated by BioTrib’s Early Stage Researchers.
Dilesh is researching the Development of 3D-printable, self-lubricated polymer composites with improved wear resistance for total joint replacement at Luleå University of Technology, Sweden.
References:
[1] D. Dowson, “Bio-tribology,” Faraday Discuss, vol. 156, no. 0, pp. 9–30, Jul. 2012, doi: 10.1039/C2FD20103H.
[2] D. J. Groen and A. Unsworth, “Tribology of Human and Artificial Joints,” http://dx.doi.org/10.1243/PIME_PROC_1991_205_287_02, vol. 205, no. 3, pp. 163–172, Aug. 2016, doi: 10.1243/PIME_PROC_1991_205_287_02.
[3] M. J. Furey and B. M. Burkhardt, “Biotribology: Friction, wear, and lubrication of natural synovial joints,” Lubrication Science, vol. 9, no. 3, pp. 255–271, May 1997, doi: 10.1002/LS.3010090303.
[4] R. K. Nanstad, “Encyclopedia of Materials Science and Engineering, ed. MB Bever.,” Pergamon Press, New York, 1986.
[5] C. W. McCutchen, “Lubrication of and by Articular Cartilage,” Cartilage, pp. 87–107, Jan. 1983, doi: 10.1016/B978-0-12-319503-6.50009-8.
[6] T. Murakami, H. Higaki, Y. Sawae, N. Ohtsuki, S. Moriyama, and Y. Nakanishi, “Adaptive multimode lubrication in natural synovial joints and artificial joints,” Proc Inst Mech Eng H, vol. 212, no. 1, pp. 23–35, 1998, doi: 10.1243/0954411981533791.
[7] V. C. Mow, S. C. Kuei, W. M. Lai, and C. G. Armstrong, “Biphasic Creep and Stress Relaxation of Articular Cartilage in Compression: Theory and Experiments,” J Biomech Eng, vol. 102, no. 1, pp. 73–84, Feb. 1980, doi: 10.1115/1.3138202.
[8] W. B. H. Akdy, “Boundary lubrication.—The temperature coefficient,” Proceedings of the Royal Society of London. Series A, Containing Papers of a Mathematical and Physical Character, vol. 101, no. 713, pp. 487–492, Sep. 1922, doi: 10.1098/RSPA.1922.0060.
[9] T. MURAKAMI, “The Lubrication in Natural Synovial Joints and Joint Prostheses,” JSME international journal. Ser. 3, Vibration, control engineering, engineering for industry, vol. 33, no. 4, pp. 465–474, Dec. 1990, doi: 10.1299/JSMEC1988.33.465.
[10] D. D., “Are our joint replacement materials adequate?,” Proc. Instn. Mech. Engrs, Int. Conf. The Changing Role of Engineering in Orthopaedics, 1989, vol. 1, 1989, Accessed: Jan. 17, 2023. [Online]. Available: https://cir.nii.ac.jp/crid/1573950399846027776
[11] J. Charnley, “Low Friction Principle,” Low Friction Arthroplasty of the Hip, pp. 3–15, 1979, doi: 10.1007/978-3-642-67013-8_2.
[12] Z. M. Jin and D. Dowson, “A full numerical analysis of hydrodynamic lubrication in artificial hip joint replacements constructed from hard materials,” http://dx.doi.org/10.1243/0954406991522310, vol. 213, no. 4, pp. 355–369, Aug. 2016, doi: 10.1243/0954406991522310.
[13] S. L. Smith, D. Dowson, and A. A. J. Goldsmith, “The effect of femoral head diameter upon lubrication and wear of metal-on-metal total hip replacements,” http://dx.doi.org/10.1243/0954411011533724, vol. 215, no. 2, pp. 161–170, Aug. 2016, doi: 10.1243/0954411011533724.